Hysterectomy
Physicians perform hysterectomy – the surgical removal of the uterus – to treat a wide variety of uterine conditions. Each year in the U.S. alone, doctors perform approximately 600,000 hysterectomies, making it the second most common surgical procedure.
Types of Hysterectomy
There are various types of hysterectomy that are performed depending on the patient’s diagnosis:
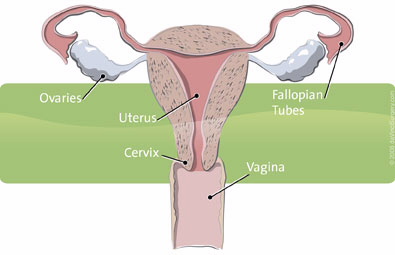
- Supracervical hysterectomy – removes the uterus, leaves cervix intact
- Total hysterectomy – removes the uterus and cervix
- Radical hysterectomy or modified radical hysterectomy – a more extensive surgery for gynecologic cancer a radical hysterectomy includes removing the uterus and cervix and may also remove part of the vagina, fallopian tubes, ovaries and lymph nodes in order to stage the cancer (determine how far it has spread).
Approaches to Hysterectomy
Surgeons perform the majority of hysterectomies using an “open” approach, which is through a large abdominal incision. An open approach to the hysterectomy procedure requires a 6-12 inch incision. When cancer is involved, the conventional treatment has always been open surgery using a large abdominal incision, in order to see and, if necessary, remove related structures like the cervix or the ovaries.
A second approach to hysterectomy, vaginal hysterectomy, involves removal of the uterus through the vagina, without any external incision or subsequent scarring. Surgeons most often use this minimally invasive approach if the patient’s condition is benign (non-cancerous), when the uterus is normal size and the condition is limited to the uterus.
In laparoscopic hysterectomies, the uterus is removed either vaginally or through small incisions made in the abdomen. The surgeon can see the target anatomy on a standard 2D video monitor thanks to a miniaturized camera, inserted into the abdomen through the small incisions. A laparoscopic approach offers surgeons better visualization of affected structures than either vaginal or abdominal hysterectomy alone.
While minimally invasive vaginal and laparoscopic hysterectomies offer obvious potential advantages to patients over open abdominal hysterectomy – including reduced risk for complications, a shorter hospitalization and faster recovery – there are inherent drawbacks. With vaginal hysterectomy, surgeons are challenged by a small working space and lack of view to the pelvic organs. Additional conditions can make the vaginal approach difficult, including when the patient has:
- A narrow pubic arch (an area between the hip bones where they come together)
- Thick adhesions due to prior pelvic surgery, such as C-section
- Severe endometriosis
- Non-localized cancer (cancer outside the uterus) requiring more extensive tissue removal, including lymph nodes
With laparoscopic hysterectomies, surgeons may be limited in their dexterity and by 2D visualization, potentially reducing the surgeon's precision and control when compared with traditional abdominal surgery.
da Vinci® Hysterectomy

A new, minimally invasive approach to hysterectomy, da Vinci Hysterectomy, combines the advantages of conventional open and minimally invasive hysterectomies – but with potentially fewer drawbacks. da Vinci Hysterectomy is becoming the treatment of choice for many surgeons worldwide. It is performed using the da Vinci System, which enables surgeons to perform surgical procedures with unmatched precision, dexterity and control. Read about what may be the most effective, least invasive approach to hysterectomy – da Vinci Hysterectomy.
- Center for Disease Control. Keshavarz H, Hillis S, Kieke B, Marchbanks P. Hysterectomy Surveillance — United States, 1994–1999. Morbidity and Mortality Weekly Report. Surveillance Summaries. July 12, 2002. Vol. 51 / SS-5. Page 1. www.cdc.gov/mmwr/PDF/ss/ss5105.pdf
- Harmanli OH, Khilnani R, Dandolu V, Chatwani AJ. Narrow pubic arch and increased risk of failure for vaginal hysterectomy. Obstet Gynecol. 2004 Oct;104(4):697-700.
- Paparella P, Sizzi O, Rossetti A, De Benedittis F, Paparella R. Vaginal hysterectomy in generally considered contraindications to vaginal surgery. Arch Gynecol Obstet. 2004 Sep;270(2):104-9. Epub 2003 Jul 10.
- Johnson N, Barlow D, Lethaby A, Tavender E, Curr L, Garry R. Methods of hysterectomy: systematic review and meta-analysis of randomised controlled trials. BMJ. 2005 Jun 25;330(7506):1478. Review.
While clinical studies support the effectiveness of the da Vinci System when used in minimally invasive surgery, individual results may vary. Surgery with the da Vinci Surgical System may not be appropriate for every individual. Always ask your doctor about all treatment options, as well as their risks and benefits.
Content provided by Intuitive Surgical. For more information on this topic, please visit www.davincisurgery.com
